
Connecting hearing aid users: it’s not the technology, it’s what people do with the technology
Dr. Melanie Ferguson explains how connected hearing healthcare technologies can supplement standard clinical practice, enabling and empowering hearing aid users.
In the pre-March 2020 days, before the dreaded ‘C’ and ‘P’ words dominated our lives, and I had the pleasure to talk at conferences in-person, I often used to ask the audiologists in the audience, “Are you confident that the information you give your new hearing aid patients is understood, absorbed and acted upon when the patients leave the comfort of your clinic room?”.
Very few hands went up.
As a translational researcher, I like to take problems identified in the clinic and find evidence-based solutions for them, often termed ‘from Bed to Bench’, or ‘reverse translation’. To address the problem of poor knowledge of hearing aids and how best to communicate, myself and a team of researchers, audiologists and patients from the UK developed C2Hear.
C2Hear is a multimedia online educational program based on learning theory that was co-designed by hearing aid users, for hearing aid users, to ensure the content was aligned to their specific needs.1
So was C2Hear clinically-effective?
Two high-quality, clinically-registered randomized controlled trials – the highest level of experimental evidence – showed a resounding “yes”.2,3 C2Hear was effective in significantly improving hearing-related knowledge and practical hearing aid handling skills, and increasing hearing aid use and self-efficacy.
Furthermore, patients liked C2Hear – rating it 9/10 for usefulness – reporting that it improved their confidence to communicate with others, and was preferred to written information.
This was supported by a Cochrane Review that showed that C2Hear was the most clinically-effective intervention to improve hearing aid use.4 As a result we have made C2Hear freely available online via YouTube, and a more recent www.c2hearonline.com.
Despite these positive results, there were limitations to C2Hear. The interactive videos (or re-usable learning objects) were long – typically between 5-8 minutes. While that was okay in 2013, when C2Hear was trialed originally, in the world of Tik Tok and Twitter, these videos are now way too long.
The videos were also a ‘one size fits all’, with limited opportunity for individuals to personalize the information they needed, when they wanted it.
To future-proof the concept, we repurposed C2Hear for mobile technologies. Videos were made shorter, more individualized, and with greater interactivity. These videos were designed to further connect hearing aid users to high-quality information and provide greater benefits. We called this mhealth educational intervention ‘m2Hear’.
m2Hear, the mobile version for first-time hearing aid users
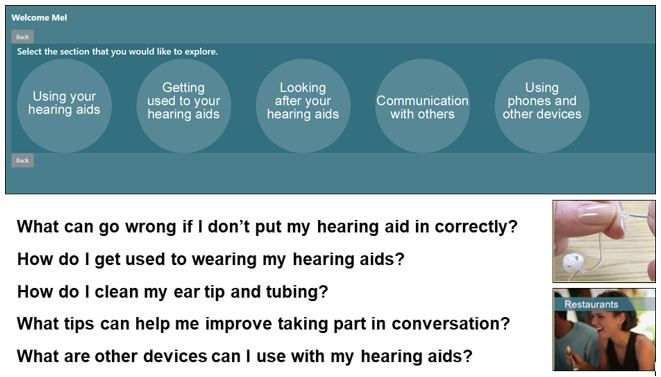
m2Hear included 42 bite-sized one minute videos. Each addressed a specific question identified as important for hearing aid users (e.g. “How do I get used to wearing my hearing aids?”), with feedback and activities. See Figure 1 for examples.
Again, we worked closely with a fantastic group of hearing aid users and a communication partner ─ our patient and public involvement (PPI) panel. We embedded participatory design, based on principles of human-technology interaction, and theoretically-grounded in health behavior change theory (COM-B model) into the development of m2Hear.5
We trialed m2Hear in 59 first-time hearing aid users from the local clinic population in Nottingham, UK. Average age was 65 years, slightly younger than the average first-time hearing aid user, most likely because we included people who owned or used mobile technologies, such as a smartphone or tablet (81% and 73% ownership respectively).
We were keen to see how user-friendly m2Hear was, as usability – or lack of – is a major barrier in digital technologies. Below are our findings:
- Usability was high at 88.5% based on the System Usability Scale, where a score ≥68% is considered average.
- There were similar results based on the uMARS, a mobile application rating scale (score range, 0-5), with very high average scores for Information (4.7) and Functionality (4.5).These ratings indicated that m2Hear was perceived by users to have high-quality and informational content from credible sources, was easy-to-use and had high performance of features, likely reflecting the participatory input from hearing aid users and our PPI panel.
- Engagement had the poorest rating at 3.6. At first glance, this was a little disappointing as we had set out our stall for greater interaction and individualization. However, it transpired that this was because the user was unable to customize the platform interface, and individual items for Interest and Target Audience were high (4.2 and 4.5 respectively).
What did our participants think of m2Hear?
Overall, our participants’ feedback was very positive. For example:
- 98% liked the short video duration
- 92% reported that if they had a problem with their hearing or hearing aids they would refer back to m2Hear, and
- 84% agreed that m2Hear had given them more confidence to use their hearing aids and communicate with others.
This was also reflected in the open-ended questions. Participants reported that m2Hear:
- was clear, concise and comprehensive
- provided useful reminders, reassurance and confidence
- was preferable to C2Hear5
Similarly, pre-post fitting outcome scores for participation in everyday life, self-efficacy, hearing ability and knowledge improved significantly, with large effect sizes (Cohens d ≥ 1.3).
This study, and others before it relating to patients, partners and professionals,6 shows that having high-quality online information provides significant benefits across a range of outcomes and participant reports. This includes improvement in self-management3 and empowerment7, which is not surprising as knowledge is core to both.8,9,
The big question is, do people use C2Hear/m2Hear in the ‘real-world’?
To date, there have been over 700,000 online views of C2Hear globally, across 50+ countries. Between February and April 2020, we saw a four-fold increase in the use of C2HearOnline, as a result of the Covid19 pandemic, as online audiology services were sought.
Now, more than ever, we are acutely aware of how CHH technologies can supplement standard clinical practice, enabling clinical audiologists to support their clients remotely.
Even before the pandemic, there was a broad consensus on embedding CHH technologies into clinical practice.10 As seen with C2HearOnline and other CHH technologies, this trend is on the increase.11
With the delayed OTC bill in the USA looking imminent, the need for high-quality online information and support is likely to increase. Particularly, if embedded in digital solutions to address other important aspects of hearing healthcare, such as social, emotional and well-being support.12
If you are an audiologist, why not check out C2Hear and m2Hear for yourself and bring this into your clinical practice. You can also add the links to your own website – you don’t need to ask. Our aim was always to make these available to whoever wants, and will benefit, from them.
One of our very first research participants beautifully described how C2Hear helped her to better manage and gain benefit from her hearing aids, “if it wasn’t for [C2Hear] I would have given up wearing my hearing aids”.
|
Background to the Connected Hearing Healthcare supplement In December 2017, I had the pleasure of meeting three US researchers at a Phonak Expert Circle on delivering audiology service through online models in Miami. There are varied terms for this (e.g. telehealth, eAudiology, teleaudiology, mhealth), however ‘Connected Hearing Healthcare’ (CHH) is a term that is increasingly being used to encompass the remote and virtual developments that are coming to the fore globally. The long and the short of that meeting was that we (Danielle Glista, Karen Munoz, Evelyn Davies-Venn) jointly guest-edited a supplement for the International Journal of Audiology on CHH,13 kindly sponsored by Phonak. Below is a summary of my contribution to this timely supplement on the feasibility of m2Hear,14 freely accessible here. |
References
- Ferguson, M., Leighton, P., Brandreth, M., & Wharrad, H. (2018). Development of a multimedia educational programme for first-time hearing aid users: A participatory design. International Journal of Audiology, 57(8), 600-609.
- Ferguson, M. A., Brandreth, M., Leighton, P., Brassington, W., & Wharrad, H. (2016). A randomized controlled trial to evaluate the benefits of a multimedia educational programme for first-time hearing aid users. Ear and Hearing, 37(2), 123-136. https://doi.org/10.1097/AUD.0000000000000237
- Gomez, R., & Ferguson, M. (2020). Improving knowledge and self-efficacy for hearing aid self-management: the early delivery of a multimedia-based education program in first-time adult hearing aid users. International Journal of Audiology, 59(4), 272-281.
- Barker, F., Mackenzie, E., Elliott, L., Jones, S., & de Lusignan, S. (2016). Interventions to Improve Hearing Aid Use in Adult Auditory Rehabilitation. The Cochrane Library.
- Maidment, D. W., Coulson, N. S., Wharrad, H., Taylor, M., & Ferguson, M. A. (2020a). The development of an mHealth educational intervention for first-time hearing aid users: combining theoretical and ecologically valid approaches. International Journal of Audiology, 59(7), 492-500.
- Ferguson, M., Maidment, D., Henshaw, H., & Gomez, R. (2019). Knowledge is power: improving outcomes for patients, partners, and professionals in the digital age. Perspectives of the ASHA Special Interest Groups, 4(1), 140-148.
- Maidment, D. W., Heyes, R., Gomez, R., Coulson, N. S., Wharrad, H., & Ferguson, M. A. (2020b). Evaluating a theoretically informed and cocreated mobile health educational intervention for first-time hearing aid users: qualitative interview study. JMIR mhealth and uhealth, 8(8), e17193.
- Convery, E., Hickson, L., Meyer, C., & Keidser, G. (2019). Predictors of hearing loss self-management in older adults. Disability and Rehabilitation, 41(17), 2026-2035.
- Gotowiec, S., Larsson, J., Incerti, P., Young, T., Smeds, K., Wolters, F., Herrlin, P., & Ferguson, M. (2021). Understanding patient empowerment along the hearing health journey. International Journal of Audiology, 1-11.
- Olson, A., Maidment, D. W., & Ferguson, M. A. (2021). Consensus on connected hearing health technologies and service delivery models in the UK: a Delphi review. International Journal of Audiology, 1-8.
- Eikelboom, R. H., Bennett, R. J., Manchaiah, V., Parmar, B., Beukes, E., Rajasingam, S. L., & Swanepoel, D. W. (2021). International survey of audiologists during the COVID-19 pandemic: use of and attitudes to telehealth. International Journal of Audiology, 1-10.
- Bennett, R. J., Barr, C., Montano, J., Eikelboom, R. H., Saunders, G. H., Pronk, M., Preminger, J. E., Ferguson, M., Weinstein, B., & Heffernan, E. (2021). Identifying the approaches used by audiologists to address the psychosocial needs of their adult clients. International Journal of Audiology, 60(2), 104-114.
- Glista, D., Ferguson, M., Muñoz, K., & Davies-Venn, E. (2021). Connected hearing healthcare: shifting from theory to practice. International Journal of Audiology, 60, Supp1, S1-S3.
- Ferguson, M. A., Maidment, D. W., Gomez, R., Coulson, N., & Wharrad, H. (2021). The feasibility of an m-health educational programme (m2Hear) to improve outcomes in first-time hearing aid users. International Journal of Audiology, 60, S30-S41.